Research challenges long-held view of early-stage Alzheimer's disease

Gerold Schmitt-Ulms, a professor in the Temerty Faculty of Medicine's department of laboratory medicine and pathology, was one of the authors of the new study (supplied image)
Published: July 4, 2023
Recent research from the Tanz Centre for Research in Neurodegenerative Diseases in the University of Toronto's Temerty Faculty of Medicine is challenging long-held views of how a hormone called somatostatin influences the earliest stages of Alzheimer’s disease.
“Importantly, for the first time, this research indicates the extent to which somatostatin could be important in Alzheimer’s disease,” says Gerold Schmitt-Ulms, co-author of the study published in Scientific Reports.
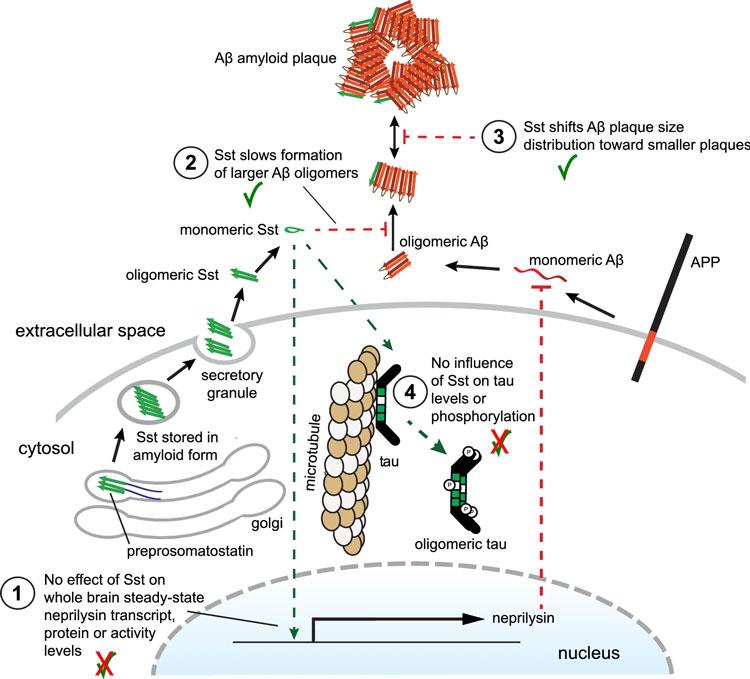
“The answer is that somatostatin has a significant effect, but it’s not black or white. It doesn’t prevent clumping of the amyloid beta protein, but slows it down. This is important, but we don’t know what this means for treatment yet,” says Schmitt-Ulms, an investigator at the Tanz Centre and professor in U of T’s department of laboratory medicine and pathology.
The dominant hypothesis of how Alzheimer's disease begins – the amyloid cascade hypothesis – says that too much amyloid beta protein is produced, which clumps together to form oligomers (small clumps of varying numbers of amyloid beta monomeric building blocks), which then continue to accumulate to form larger plaques that damage neurons.
As early as the 1970s, researchers observed that brains of people with Alzheimer’s disease had lower levels of the hormone somatostatin than people who did not have Alzheimer’s, and that the plaques of amyloid beta that are characteristic of the disease tend to form near neurons that produce somatostatin.
These observations suggested a relationship between somatostatin and amyloid beta aggregation, but researchers did not know what it was.
Then, in the early 2000s, a team from Japan published research describing that somatostatin drives production of an enzyme called neprilysin that can degrade amyloid beta. This finding suggested that if somatostatin was decreased, the levels of neprilysin would decrease – without neprilysin to degrade amyloid beta, the plaques would continue to grow, and Alzheimer's disease would progress.
This understanding of the role of somatostatin is where the field stood for more than a decade.
Several years ago, Schmitt-Ulms and his team investigated amyloid beta in its monomer and oligomer forms, specifically looking for molecules in the brain that would bind to the toxic oligomeric forms. They found that, of all proteins in the brain, somatostatin was the smallest to bind to amyloid beta – and the most selective, as it only interacted with the oligomers.
They then observed that somatostatin blocked the formation of oligomers, with higher concentrations of somatostatin having a greater effect. This earlier study provided the first evidence that somatostatin interacts directly with the oligomeric amyloid beta that are known to be the earliest stages of Alzheimer's disease, providing an alternative perspective on the impact of somatostatin on the disease.
“We didn’t actually intend to work on somatostatin, but these results made us very curious about what would happen if somatostatin was absent in an animal model that was genetically engineered to develop amyloid beta aggregations,” Schmitt-Ulms explains.
To answer this question, the research team crossed a somatostatin-deficient mouse line with an amyloidosis mouse model.
They found that when somatostatin was absent, there were more amyloid beta aggregates, consistent with what is seen in Alzheimer’s disease in humans.
Remarkably, the result did not seem to be caused by an effect of somatostatin on neprilysin levels, as there were no differences – a contradiction to the long-held understanding of the mechanism through which somatostatin impacts Alzheimer’s disease. Instead, the data suggested that somatostatin blocks oligomer formation independent of neprilysin by interacting with amyloid beta.
“There isn’t a lot of literature that explains how the environment in the brain can promote or inhibit amyloid beta forming into oligomers, so this is a nice vignette that shows that one molecule – somatostatin – seems to influence that first small oligomeric aggregation step,” Schmitt-Ulms says.
“And if you get fewer of these oligomeric forms, then you get fewer of the small clumps, which are the next step of amyloid beta aggregation – so the process made sense, and it was a striking finding.”
While the results have challenged the conventional view of somatostatin in Alzheimer’s and prompted discussions in the scientific community, what they mean for treatment is still uncertain.
Somatostatin plays important roles in the gastrointestinal, endocrine and nervous systems, so selectively promoting its role in blocking amyloid aggregation would be challenging. Schmitt-Ulms says that it is also unclear whether augmenting somatostatin, and thereby arresting the growth of amyloid beta aggregates, is beneficial.
Still, the results have shaken up the research field.
“The evidence speaks for itself, and we stand by our conclusions, but the data can’t answer what this means for therapeutics,” Schmitt-Ulms says.
“They do, however, indicate that somatostatin – one of the first-ever molecules that were biochemically linked to Alzheimer’s disease – may play a different role in the earliest stages of the disease than expected, and that in itself is important.”
The study was supported by Alberta Innovates Bio Solutions, Ontario Centres for Excellence/MaRS Innovation and the Borden Rosiak family.


